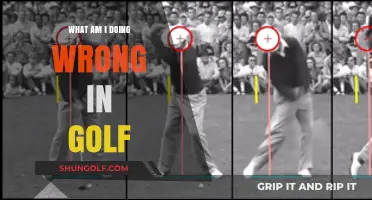
Golfer's elbow, medically known as medial epicondylitis, is a condition characterized by pain and inflammation where the tendons of the forearm muscles attach to the bony bump on the inside of the elbow (the medial epicondyle). The anatomy involved primarily includes the flexor-pronator muscle group, which consists of muscles responsible for wrist and finger flexion and forearm pronation. Key muscles affected are the flexor carpi radialis, palmaris longus, flexor carpi ulnaris, and pronator teres. Overuse or repetitive stress, often from activities like golf, tennis, or manual labor, can lead to microtears and degeneration in these tendons, causing pain and tenderness at the medial epicondyle. Understanding this anatomical involvement is crucial for diagnosing, treating, and preventing golfer's elbow.
| Characteristics | Values |
|---|---|
| Condition Name | Golfer's Elbow (Medial Epicondylitis) |
| Location | Inner side of the elbow (medial epicondyle of the humerus) |
| Affected Tissues | Tendons of the forearm muscles (wrist flexors and pronators) |
| Primary Muscles Involved | Pronator teres, flexor carpi radialis, flexor carpi ulnaris, palmaris longus |
| Common Causes | Repetitive wrist, hand, or forearm movements (e.g., golfing, throwing) |
| Symptoms | Pain, tenderness, stiffness, weakness in the elbow and forearm |
| Nerve Involvement | Ulnar nerve (may be compressed, causing tingling or numbness) |
| Diagnosis | Physical examination, imaging (X-ray, MRI) if necessary |
| Treatment | Rest, ice, physical therapy, anti-inflammatory medications, bracing |
| Prevention | Proper technique, strengthening exercises, ergonomic adjustments |
| Chronic Risks | Tendon degeneration, chronic pain, reduced grip strength |
Explore related products






What You'll Learn
- Medial Epicondyle: Involvement of the bony bump on the inner elbow where tendons attach
- Flexor Tendons: Overuse or strain of tendons connecting forearm muscles to the medial epicondyle
- Pronator Teres Muscle: Inflammation or injury to this forearm muscle contributing to golfer’s elbow
- Wrist Flexor Muscles: Strain on muscles responsible for bending the wrist, often overworked in golf
- Ulnar Nerve: Compression or irritation of the nerve near the medial epicondyle causing pain
![]()
Medial Epicondyle: Involvement of the bony bump on the inner elbow where tendons attach
Golfer's elbow, medically known as medial epicondylitis, is a condition characterized by pain and inflammation where the tendons of the forearm attach to the bony bump on the inner elbow, known as the medial epicondyle. This bony prominence serves as a critical attachment site for several muscles responsible for wrist and finger flexion, as well as forearm pronation. The medial epicondyle is a vital anatomical structure because it provides the anchor point for the tendons of the flexor-pronator muscle group, which includes muscles like the flexor carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis, and pronator teres. When these tendons are subjected to repetitive stress or overuse, they can become irritated, leading to the symptoms associated with golfer's elbow.
The involvement of the medial epicondyle in golfer's elbow is directly related to its role as the origin of these forearm muscles. Repetitive gripping, swinging, or throwing motions—common in activities like golf, tennis, or manual labor—can strain the tendons at their attachment point on the medial epicondyle. Over time, this strain causes microtears and inflammation in the tendon fibers, resulting in pain and tenderness over the inner elbow. The pain may radiate along the inner forearm and worsen with gripping or wrist movements, as these actions place increased tension on the affected tendons and their insertion on the medial epicondyle.
Anatomically, the medial epicondyle is part of the distal humerus, the lower end of the upper arm bone. Its location makes it susceptible to injury in activities that involve forceful or repetitive wrist and finger flexion. Unlike the lateral epicondyle, which is involved in tennis elbow, the medial epicondyle’s tendon attachments are more prone to stress in activities requiring strong gripping or repetitive bending of the wrist toward the palm. Understanding this anatomical relationship is crucial for diagnosing and treating golfer's elbow, as it highlights the need to address the specific tendons and muscles attached to this bony landmark.
To manage golfer's elbow, it is essential to reduce the strain on the tendons attached to the medial epicondyle. This can be achieved through rest, activity modification, and targeted strengthening exercises for the flexor-pronator muscles. Physical therapy often focuses on improving the flexibility and strength of these muscles to distribute force more evenly across the tendon attachment site. In severe cases, treatments such as bracing, anti-inflammatory medications, or corticosteroid injections near the medial epicondyle may be considered to alleviate pain and inflammation.
Preventing golfer's elbow involves protecting the medial epicondyle and its associated tendons from overuse. This includes using proper technique in sports or work activities, incorporating ergonomic tools, and gradually increasing the intensity of repetitive motions. Stretching and strengthening exercises for the forearm muscles can also help maintain the health of the tendons at the medial epicondyle, reducing the risk of injury. By focusing on the anatomical involvement of the medial epicondyle, individuals can better understand the mechanics of golfer's elbow and take proactive steps to prevent or address this condition effectively.
Master Your Golf Swing: Proven Tips to Avoid Double Cross
You may want to see also
Explore related products






![]()
Flexor Tendons: Overuse or strain of tendons connecting forearm muscles to the medial epicondyle
Golfer's elbow, medically known as medial epicondylitis, is a condition characterized by pain and inflammation where the tendons of the forearm muscles attach to the bony bump on the inside of the elbow (the medial epicondyle). Among the anatomical structures involved, the flexor tendons play a central role. These tendons connect the forearm muscles responsible for wrist and finger flexion to the medial epicondyle. Overuse or strain of these tendons is a primary cause of golfer's elbow, leading to microtears, degeneration, and chronic pain.
The flexor tendons involved in golfer's elbow are part of the common flexor tendon, which comprises the tendons of several muscles, including the flexor carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis, and palmaris longus. These muscles are essential for bending the wrist, curling the fingers, and gripping objects. Repetitive or excessive use of these muscles, such as in golfing, throwing, or manual labor, places significant stress on the flexor tendons where they attach to the medial epicondyle. Over time, this repetitive stress can lead to tendon overuse, inflammation, and degeneration, resulting in the symptoms of golfer's elbow.
The mechanism of injury in golfer's elbow often involves eccentric contraction of the flexor muscles, which occurs when the muscles lengthen under load. For example, in the follow-through of a golf swing or during heavy lifting, the flexor tendons are stretched while under tension, causing microscopic damage. This cumulative damage weakens the tendon fibers and impairs their ability to heal, leading to chronic tendinopathy. The medial epicondyle, being the site of tendon attachment, becomes the focal point of pain and tenderness.
Diagnosis of flexor tendon overuse or strain typically involves a physical examination, where pressure applied to the medial epicondyle reproduces pain. Additionally, specific tests, such as the flexion-based resisted wrist and finger tests, may be performed to isolate the affected tendons. Imaging studies like ultrasound or MRI can further confirm tendon inflammation or degeneration. Treatment focuses on reducing inflammation, alleviating pain, and promoting tendon healing. Rest, ice, anti-inflammatory medications, and physical therapy are first-line interventions. In severe cases, corticosteroid injections or surgical decompression may be considered to relieve symptoms and restore function.
Preventing golfer's elbow involves addressing the underlying causes of flexor tendon strain. This includes proper technique in sports or activities, gradual progression in intensity and duration, and adequate rest to allow tendon recovery. Strengthening the forearm muscles and improving flexibility can also reduce the risk of overuse injuries. By understanding the role of the flexor tendons and their connection to the medial epicondyle, individuals can take proactive steps to protect their elbow health and prevent the development of golfer's elbow.
Leather Golf Gloves: Better or Not?
You may want to see also
Explore related products

![Sparthos Elbow Compression Sleeves [Flamingo Pink - Small] x Tennis Elbow Brace [Pack of 2]](https://m.media-amazon.com/images/I/71JTrqTOA+L._AC_UL320_.jpg)




![]()
Pronator Teres Muscle: Inflammation or injury to this forearm muscle contributing to golfer’s elbow
The Pronator Teres muscle plays a significant role in the development and persistence of golfer's elbow, a condition medically known as medial epicondylitis. This muscle, located in the forearm, is responsible for pronation, the movement that turns the palm of the hand downward. It originates from the medial epicondyle of the humerus and inserts into the middle of the radius bone. When the Pronator Teres becomes inflamed or injured, it can contribute to the pain and discomfort associated with golfer's elbow. This inflammation often arises from repetitive strain or overuse, particularly in activities that involve gripping, twisting, or throwing, such as golf, hence the name "golfer's elbow."
Inflammation or injury to the Pronator Teres muscle typically occurs due to the cumulative effect of repetitive motions that stress the forearm muscles and tendons. In golfers, the repeated swinging of the club places significant strain on the medial forearm structures, including the Pronator Teres. Over time, this can lead to microtears in the muscle fibers and tendon attachments, resulting in inflammation and pain. The Pronator Teres is particularly vulnerable because it works in conjunction with other wrist flexors and pronators during the golf swing, amplifying the stress on this specific muscle group.
Symptoms of Pronator Teres inflammation or injury include pain on the inner side of the elbow, which may radiate into the forearm. Individuals may also experience tenderness when pressing on the medial epicondyle or weakness in gripping and pronation movements. Diagnosis often involves a physical examination, where a healthcare provider assesses pain levels during specific movements, such as resisted pronation. Imaging studies like ultrasound or MRI may be used to confirm the extent of inflammation or damage to the Pronator Teres and surrounding tissues.
Treatment for Pronator Teres-related golfer's elbow focuses on reducing inflammation, alleviating pain, and restoring function. Initial management includes rest, ice application, and anti-inflammatory medications to minimize swelling and discomfort. Physical therapy is a cornerstone of treatment, involving stretching and strengthening exercises to improve flexibility and reduce strain on the muscle. Therapists may also use techniques like manual therapy or ultrasound to promote healing. In severe cases, corticosteroid injections or surgical intervention may be considered to address chronic inflammation or tendon damage.
Preventing Pronator Teres inflammation involves modifying activities to reduce repetitive strain and incorporating ergonomic adjustments. For golfers, this may mean refining their swing technique to minimize stress on the forearm muscles or using equipment with proper grip size and flexibility. Strengthening exercises targeting the forearm muscles, including the Pronator Teres, can also enhance resilience to injury. Additionally, gradual progression in activity intensity and adequate warm-up routines are essential to prevent overuse injuries. By addressing the specific demands placed on the Pronator Teres, individuals can effectively manage and prevent golfer's elbow associated with this muscle.
Golf Terms: Their Historical Origins and Etymology
You may want to see also
Explore related products






![]()
Wrist Flexor Muscles: Strain on muscles responsible for bending the wrist, often overworked in golf
Golfer's elbow, medically known as medial epicondylitis, is a condition characterized by pain and inflammation where the tendons of the forearm muscles attach to the bony bump on the inside of the elbow. Among the anatomical structures involved, the wrist flexor muscles play a significant role. These muscles, responsible for bending the wrist and assisting in gripping actions, are often overworked in activities like golf, leading to strain and injury. The primary wrist flexor muscles include the flexor carpi radialis, flexor carpi ulnaris, and palmaris longus, all of which originate on the medial epicondyle of the humerus and insert into the bones of the hand and wrist.
In the context of golf, the repetitive motion of swinging a club places considerable stress on these muscles. During the downswing and follow-through, the wrist flexors are engaged to maintain grip and control the club, often under significant force. Over time, this repetitive action can lead to microtears in the tendons where they attach to the medial epicondyle, resulting in inflammation and pain. The strain is exacerbated by improper technique, overuse, or inadequate conditioning, making golfers particularly susceptible to this type of injury.
The flexor carpi radialis and flexor carpi ulnaris are especially vulnerable due to their direct involvement in wrist flexion and stabilization. These muscles work in tandem to flex the wrist and assist in ulnar and radial deviation, movements essential for a smooth golf swing. When overworked, the tendons of these muscles become irritated, leading to the chronic pain associated with golfer's elbow. Additionally, the palmaris longus, though less directly involved in wrist flexion, contributes to overall forearm tension and can further strain the medial epicondyle when overused.
Preventing strain on the wrist flexor muscles requires a combination of proper technique, strength training, and flexibility exercises. Golfers should focus on maintaining a neutral wrist position during the swing to minimize excessive flexion. Incorporating forearm strengthening exercises, such as wrist curls and grip training, can help build resilience in these muscles. Stretching the wrist flexors post-activity can also alleviate tension and reduce the risk of injury. By addressing the demands placed on these muscles, golfers can mitigate the strain that often leads to medial epicondylitis.
In summary, the wrist flexor muscles are central to the development of golfer's elbow due to their role in bending the wrist and their frequent engagement in the golf swing. Overworking these muscles through repetitive motion and improper technique can result in tendon strain and inflammation at the medial epicondyle. Understanding the anatomy and function of these muscles is crucial for implementing preventive measures, such as technique adjustments and targeted exercises, to reduce the risk of injury and maintain optimal performance on the course.
The Evolution of Ladder Golf: A Historical Perspective
You may want to see also
Explore related products






![]()
Ulnar Nerve: Compression or irritation of the nerve near the medial epicondyle causing pain
The ulnar nerve plays a significant role in the development of golfer's elbow, a condition characterized by pain and discomfort on the inner side of the elbow. This nerve, one of the three main nerves in the arm, runs from the neck down to the hand, providing sensation and motor function to the forearm and hand. As it travels through the elbow, the ulnar nerve passes close to the medial epicondyle, a bony prominence on the inner side of the elbow. In the context of golfer's elbow, compression or irritation of the ulnar nerve at this specific location can lead to a range of symptoms.
When the ulnar nerve is compressed or irritated near the medial epicondyle, it can result in a condition known as cubital tunnel syndrome, which often coexists with golfer's elbow. This compression may occur due to various factors, including repetitive motions, direct trauma, or prolonged pressure on the elbow. For instance, golfers who repeatedly swing their clubs with excessive force or improper technique can put excessive strain on the medial elbow structures, leading to inflammation and subsequent compression of the ulnar nerve. The nerve's proximity to the medial epicondyle makes it vulnerable to such issues.
The symptoms of ulnar nerve compression or irritation in golfer's elbow can vary. Patients often experience pain along the inner elbow, which may radiate down the forearm and into the hand. This pain can be accompanied by numbness, tingling, or a "pins and needles" sensation in the ring and little fingers, as these digits receive sensory innervation from the ulnar nerve. In more severe cases, muscle weakness in the hand and a decreased grip strength may develop, affecting the patient's ability to perform fine motor tasks.
Diagnosing ulnar nerve involvement in golfer's elbow typically involves a thorough physical examination. A doctor may perform specific tests, such as the Tinel's sign, where tapping over the nerve at the elbow reproduces the symptoms, indicating irritation. Additionally, nerve conduction studies and electromyography can help confirm the diagnosis and assess the severity of nerve compression. Treatment options focus on relieving pressure on the nerve and managing inflammation. This can include rest, bracing or splinting to immobilize the elbow, anti-inflammatory medications, and physical therapy to stretch and strengthen the surrounding muscles.
In chronic or severe cases, where conservative treatments fail to provide relief, surgical intervention might be considered. The goal of surgery is to decompress the ulnar nerve, providing it with more space and reducing irritation. This can be achieved through various techniques, such as medial epicondylectomy, where a small portion of the medial epicondyle is removed to create more room for the nerve, or ulnar nerve transposition, which involves moving the nerve to a new location to reduce tension and compression. Post-surgical rehabilitation is crucial to ensure a full recovery and prevent future complications.
Easy DIY Guide: Replacing Your Golf Cart Mirror Cover Step-by-Step
You may want to see also
Frequently asked questions
Golfer's elbow, or medial epicondylitis, is a condition causing pain where the tendons of the forearm muscles attach to the bony bump on the inside of the elbow (medial epicondyle). It primarily involves the flexor-pronator tendons, which control wrist and finger flexion and forearm rotation.
The muscles most commonly involved are the wrist flexors (flexor carpi radialis and flexor carpi ulnaris) and the pronator teres. These muscles originate at the medial epicondyle and are responsible for bending the wrist and rotating the forearm.
The medial epicondyle is the bony prominence on the inner side of the elbow where the flexor-pronator tendons attach. Overuse or repetitive stress can cause inflammation or microtears in these tendons at their attachment site, leading to pain and tenderness in this area.
While golfer's elbow primarily affects tendons, the ulnar nerve, which runs near the medial epicondyle, can sometimes be irritated due to inflammation or swelling in the area. This may cause additional symptoms like tingling or numbness in the hand, though it is not the primary focus of the condition.